Enough of the errors – we need courageous people to take truly courageous steps to stop healthcare worker harms – Part 1
Our latest blog from our Infection Prevention and Control Advisor, Dr Evonne T Curran, reflects on the need for decision-makers to be truly courageous. It will be published in two parts/
If you could write a blog on errors, said Alison. I did. I wrote a blog and then thought what’s the point of that. I have written many blogs, papers and reports on errors since shortly after this 5 year old pandemic began. Decision-makers made errors and everyone knows it – the problem is their perpetuation. So, against Alison’s request this blog is about truly courageous steps to reducing harms and improving safety. My efforts in appealing to the great and the good, have had less impact than a feather falling on wet concrete. To be clear, this has never been about blame or retribution. This has always been about decision-makers making better decisions and stopping harms.
So, here are 10 Infection Prevention and Control (IPC) truly courageous next steps. Something for the decision-makers to ponder instead of perpetually kicking cans down the road with options limited to rocks and hard places. The plea of the blog is for decision-makers to be positive, be courageous and reduce the burdens of COVID on healthcare now and in the future.
Truly Courageous Step 1 – Acknowledge the Mode of Transmission is predominantly airborne
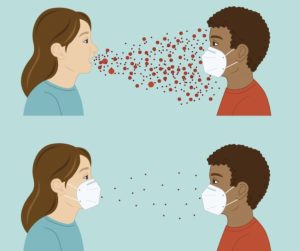
In the way bloodletting was wrongly used to treat almost every disease, droplets were used to explain every respiratory infection transmission unless far-afield spread was proven. Aerosol scientists have shown that most respiratory transmission happens when exhaled aerosols containing pathogens are inhaled by a susceptible person. The IPC profession entered the pandemic with a definition of respiratory transmission that “defied physics” (Marr & Tang 2021). There is no scientific sleight of hand that can negate the need for IPC pandemic-decision makers and guidance authors to say that their understanding of transmission was wrong and accept now that most respiratory infections arise following inhalation.
Truly Courageous Step 2 – Admitting Aerosol Generating Procedures (AGPs) did not turn sprayed on droplets into infections that were inhaled
 This situation arose from the embers of the SARS1 outbreak in which healthcare workers (HCWs) assisting with AGPs were found to be at higher risk of acquiring SARS1. However, aerosol scientists showed that coughing generates up to 400 times more aerosols than some AGPs. The reason AGPs were associated with acquisition was due to confounding factors. HCWs undertaking AGPs were close to infectious symptomatic people for periods of time, during which they inhaled the pathogen laden aerosols. So, the truly courageous step 2 is to both admit this error and reconsider the entire basis for the NIPCM as AGPs do not turn sprayed on droplets into inhaled aerosols.
This situation arose from the embers of the SARS1 outbreak in which healthcare workers (HCWs) assisting with AGPs were found to be at higher risk of acquiring SARS1. However, aerosol scientists showed that coughing generates up to 400 times more aerosols than some AGPs. The reason AGPs were associated with acquisition was due to confounding factors. HCWs undertaking AGPs were close to infectious symptomatic people for periods of time, during which they inhaled the pathogen laden aerosols. So, the truly courageous step 2 is to both admit this error and reconsider the entire basis for the NIPCM as AGPs do not turn sprayed on droplets into inhaled aerosols.
Truly Courageous Step 3 – Acknowledge where the HCW acquisition risks are high
Staff in ITU became the iconic image of the early pandemic where HCWs were top-to-toe in PPE working tirelessly to stop the seriously ill from dying. AGPs were frequently done in the ITU. However, this is not where the nosocomial risk was greatest. By the time patients had progressed from first symptom to ICU, many days of infectiousness had passed. More infectious, but not recognised as such, were symptomatic patients at earlier stages of their illness who required prolonged personal, but not intensive, care. HCWs close to infectious, symptomatic people for long periods of time were significantly exposed. So, whilst the ITU staff in better ventilated spaces, had effective RPE, healthcare workers were caring for highly infectious people, in less well-ventilated areas, with inadequate RPE for long periods of time. Acknowledging this under recognised risk is perhaps the most important courageous step. It leads to the need to make the air quality visible.
Truly Courageous Step 4 – Accept the current guidance production model is inadequate for IPC guidance

During the Inquiry, Dame Hallett held up a surgical mask and an N95 and asked a question on equivalence. The response was “the evidence was weak.” This was a misinterpretation of the value of mechanistic evidence. Mechanistic evidence is used to demonstrate safety efficacy and is considered (outside of healthcare) a more reliable methodology than RCTs. For example, the safety of planes, seatbelts, condoms, cars, electric saws, and Respiratory Protection Masks is achieved and demonstrated by mechanistic evidence. The question “Do respiratory protection masks prevent the inhalation of virus better than surgical masks?” Had been asked and answered by the HSE who emphatically concluded – Yes. However, umbrellas do not work if they are not used when it rains.
The truly courageous step here is to revisit guidance production methods and recommend mechanistic evidence to answer questions regarding physical safety and how transmission happens. [As an example of its importance, mechanistic evidence showed how surgical site infections began in theatre when sterile areas of the body were opened and pathogens from the air fell in.] This evidence could never have been determined by RCTs.
Truly Courageous Step 5 – don’t make decisions because you don’t like the outcomes
 A secondary mask error arose over the perception that masks caused “harms”, thereby there was no rush to recommend them. In his book Think Again, Adam Grant argues that you should not base a decision on whether you like the outcome. To the question do HCWs need RPE? The evidenced answer was – yes. The next question should have been – How do we provide HCWs with RPE and ensure their comfort and an absence of harms? Instead, the problem of inadequate RPE resulting in HCW (and patient) acquisition (a far greater harm) is yet to be solved.
A secondary mask error arose over the perception that masks caused “harms”, thereby there was no rush to recommend them. In his book Think Again, Adam Grant argues that you should not base a decision on whether you like the outcome. To the question do HCWs need RPE? The evidenced answer was – yes. The next question should have been – How do we provide HCWs with RPE and ensure their comfort and an absence of harms? Instead, the problem of inadequate RPE resulting in HCW (and patient) acquisition (a far greater harm) is yet to be solved.
Part 2 of this blog coming soon.

 This situation arose from the embers of the SARS1 outbreak in which healthcare workers (HCWs) assisting with AGPs were found to be at higher risk of acquiring SARS1. However, aerosol scientists showed that coughing generates
This situation arose from the embers of the SARS1 outbreak in which healthcare workers (HCWs) assisting with AGPs were found to be at higher risk of acquiring SARS1. However, aerosol scientists showed that coughing generates 
 A secondary mask error arose over the perception that masks caused “harms”, thereby there was no rush to recommend them. In his book
A secondary mask error arose over the perception that masks caused “harms”, thereby there was no rush to recommend them. In his book 
Angela says:
Yes! Much needed review and redirection! Healthcare workers and hospital admin staff followed the requirements for masking and goggling but only surgical masks provided so I bought my own n95s. And why did majority of staff think it ok to gather unmasked in the cafeteria? I ate outside or in a quiet no-traffic location. Step up to the challenge of following the science, decision-makers!