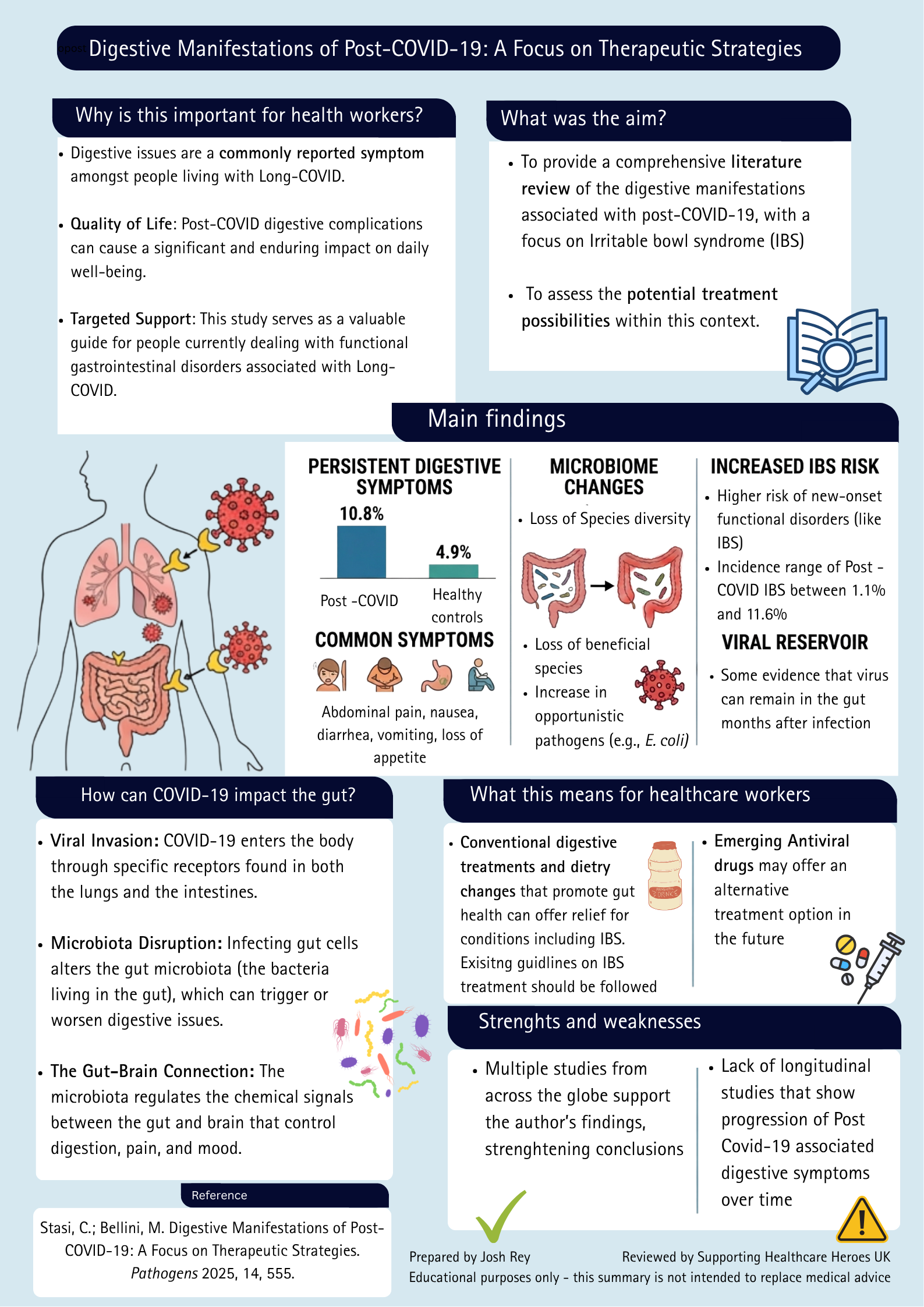
Long COVID and Digestive Symptoms: What the Research Tells Us
Research summary exploring digestive manifestations of Long COVID, including gut microbiome changes, IBS risk and potential treatment approaches.
Read more

Summary
Dr. Evonne Curran critiques WHO/CDC guidance, showing COVID droplet claims lack evidence and transmission is airborne.
This week’s blog is written by Dr Evonne Curran (@EvonneTCurran).
A Twitter friend has asked me to write a piece providing evidence that COVID is airborne. That’s not a problem; it’s the 800-word limitation that makes this challenging. So, consider this part 1.
We started the pandemic with modes of transmission, that both defied physics and were unevidenced. I have a continuous Infection Prevention and Control (IPC) career that began in the late 1980s – when it was still only ‘infection control’. The instructions at the beginning were both generic – do what you can with what you have [there’s no money] – and specific – don’t let there be another case of Legionnaires’ disease. Glasgow Royal Infirmary had had its share of Legionella outbreaks (cooling towers, humidifiers and even fire hydrants). Regarding the generic, there was never enough of anything: single rooms, wash-hand basins, equipment, means to decontaminate stuff, curtains to change etc., etc. Solutions rarely eliminated risk, and often created new ones, e.g., the introduction of more wash-hand basins brought with it microbial splash risks. We reached a nadir that created change and brought in targets, responsible persons, and inspections. However, although results improved, challenges still increased and the omnipresent outbreak risks and undervalued outbreak preparedness work was not the priority it needed to be. Thus, in this task-saturated environment the high-reliability characteristic of a preoccupation with failure went unprobed. There was also another reason, IPC teams felt assured that the guardians of definitions and guidance the World Health Organization (WHO), and the Centers for Disease Control and Prevention (CDC), would base their statements on evidence. They had access to every resource, surely, they would not fumble.
It is difficult to retrospectively identify the Modes of Transmission (MoT) involved in an outbreak. Ethics (usually) prevents confirmation of a MoT through randomised controlled trials (RCTs). Thus, the evidence needed to demonstrate transmission of a particular MoT will come from a mixture of sources: outbreaks, experimental studies, and Sherlock Holmes. Sherlock Holmes’ said: “When [or more realistically if] you have eliminated the impossible, that which remains however improbable must include* the truth”. Outbreak investigators eliminate the impossible MoTs. This is elegantly demonstrated here where, the mechanistic evidence showed tuberculosis (TB) was airborne (without RCTs). Researchers placed caged guinea pigs in the air vents above the ward ceilings; and the guinea pigs acquired the patients’ TB. This evidence demonstrated TB – in this instance – was transmitted via the air outwith a ‘close space’ because of what could be eliminated. TB could not have been spread:
Therefore, TB was adjudged to be transmitted via airborne transmission outwith a ‘close space’ otherwise known as far-afield transmission.
Ok, but first let us talk about the absence of evidence for ‘droplets’. Since everyone looked to the WHO and CDC for guidance, let’s examine both their guidance and definitions and evaluate the evidence they presented. The standard we need to verify definitions is this: there must be specifics of how the pathogen gets out, how it gets about, and how it enters to cause infection. Most importantly there must be evidence.
The WHO produced their pandemic preparedness document in 2014, (i.e., after SARS1 and MERS). It is this document to which the WHO referred when they discussed SARS-CoV-2 MoTs, e.g. WHO July 2020 statement on transmission. Statements how to differentiate between droplets and aerosols are provided therein. The critical thing here is this; the WHO wrote:
“the definitions and classification of the different types of infectious respiratory aerosols are evolving, and the implications for IPC measures are not yet clear. However, for the purpose of this document infectious respiratory aerosols are classified into:
Droplets – respiratory aerosols >5μm; and
Droplet nuclei – the residue of dried respiratory aerosols ≤5μm that results from evaporation of droplets coughed or sneezed into the atmosphere or by aerosolisation of infective material.”
For a pandemic preparedness document to state effectively we don’t know if there is a line in the sand between droplets and droplet nuclei (aerosols), but we are going to draw a line here, is an unreliable approach. Regarding droplet transmission the WHO 2014, states that droplets are propelled through the air, over short distances <1m to be deposited on the “conjunctivae, mouth, nasal, throat and pharynx”. Again, this statement is devoid of supporting citations. There is a reference to a book, but that does not contain evidence to support the statement. In another unsupported statement WHO suggested “Most of the volume (>99%) [of expired air] comprises large droplets”. However, Fennelly (2020) in one review reports that, from both breathing and coughing most particles are <4μm. Ergo, the WHO got both the size of the particles and description (they are not all evaporated droplets) wrong.
The CDC (2007) guidelines, which have been updated over time hint that the respiratory MoTs (droplets and airborne) are not supported by good evidence, e.g., ‘droplets are traditionally defined as >5μm’. The source of the evidence for the delineation between droplets and aerosols is Duguid (1946) [p17], who cites it to Hatch (1942), who does not mention a size cut off point. CDC presents one SARS1 outbreak as ‘evidence of droplets,’ but this outbreak demonstrates transmission happening in both a close space (droplet range) and several metres outwith droplet range. They should have acknowledged that the evidence from the outbreak suggests that as SARS1 transmission happens both within and outwith droplet range – SARS1 could be airborne. The erroneous assumption here is that ‘droplet range’ means ‘droplet transmission’ – but as Sherlock would say, nothing has yet been eliminated. Droplet range could also be airborne as airborne transmission happening far afield must be more likely to happen close to the source where the aerosols are densest.
Without being explicit, CDC seem to consider far-afield transmission being evidence of airborne and that happening close to a source being evidence of droplets. The WHO also seemed to be adopting a near means droplets fallacy. During the pandemic the term ‘close contact transmission’ was used to describe transmission that happened near a source but without the MoT being known. In their WHO July 2020 statement on transmission the WHO reported that SARS-CoV-2 was primarily disseminated by droplets and close contact. However, ‘close contact’ is a misnomer because ‘contact’ per se may not be involved. The schematic below shows the different ways that pathogens can spread close to a source in a non-healthcare environment in a more appropriately named ‘close space’ person-to-person transmission box (NB this is not just respiratory infections). In this close space transmission box, all MoTs are possible. Regarding the WHO’s statement 16 citations were used; however, having read them all, the only appropriate conclusion is that transmission was happening in a ‘close space’. WHO should have recognised that there was nothing to either confirm it was droplets, or exclude it being airborne.
Neither the CDC, nor the WHO evidenced the physics involved in their definitions of droplet transmission. There is no evidence that infectious particles are only transmitted in large droplets. Although evidence of droplet transmission is reported in outbreak reports, it’s still unconfirmed as airborne transmission was never excluded. There only ever was evidence of transmission happening in a close space. Thus, evidence for droplets is yet unavailable, unproven and unpublished. One assessment of this IPC droplet or airborne delineation is that it defies physics.
Part 2 will present the evidence for airborne.
* the quote is ‘must be’ the truth, but as only some MoTs are eliminated this has been altered to must ‘include’ the truth.
Research summary exploring digestive manifestations of Long COVID, including gut microbiome changes, IBS risk and potential treatment approaches.
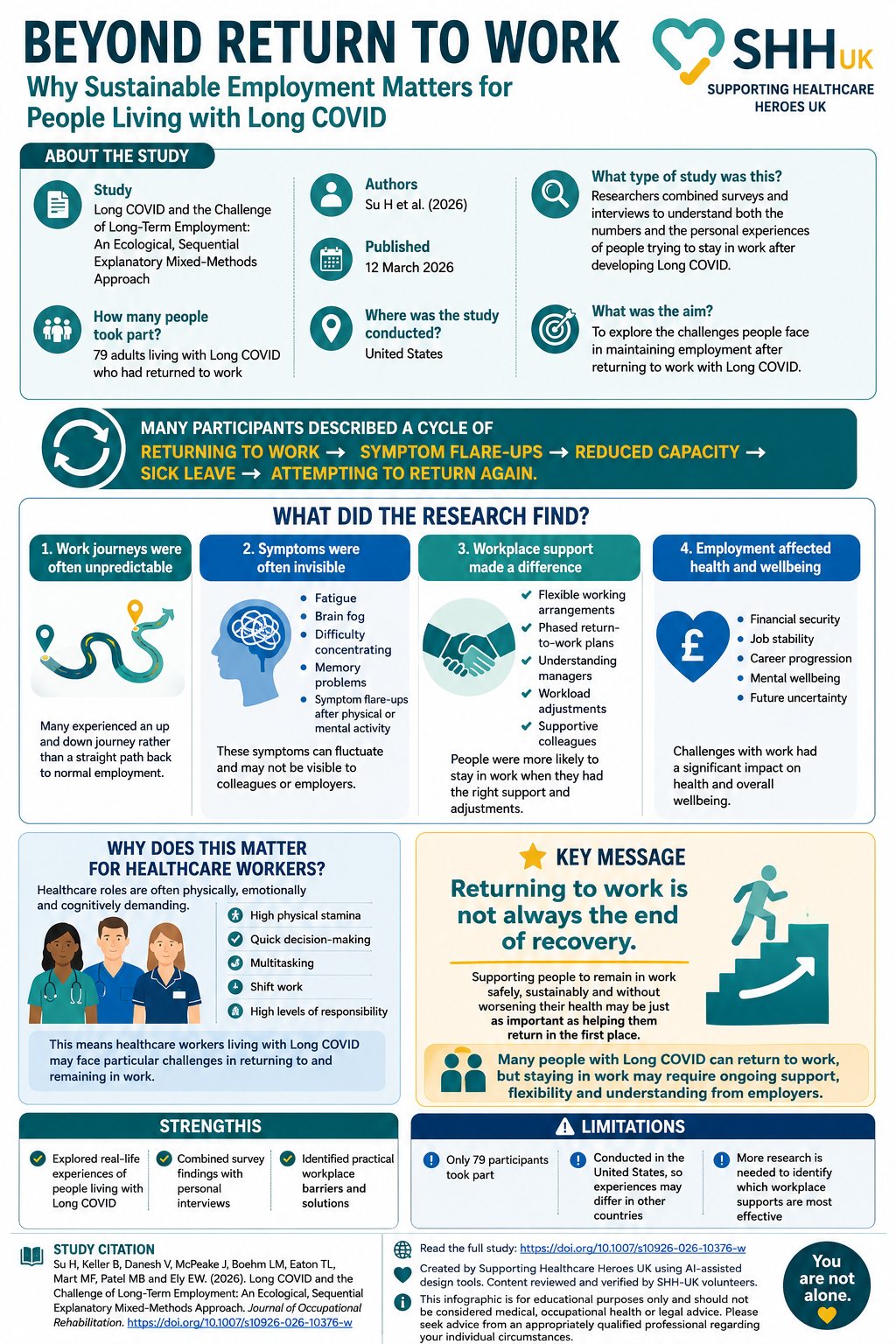
Returning to work is often viewed as a major milestone in recovery. However, for many people living with Long COVID, returning to work does not necessarily mean returning to their previous level of health. This study by Su and colleagues explored the experiences of 79 adults living with Long COVID who had returned to employment. […]
Learn why the precautionary principle is fundamental to infection prevention and how its application protects healthcare workers and patients.
Yvette Bayley says:
An interesting read, thank you.