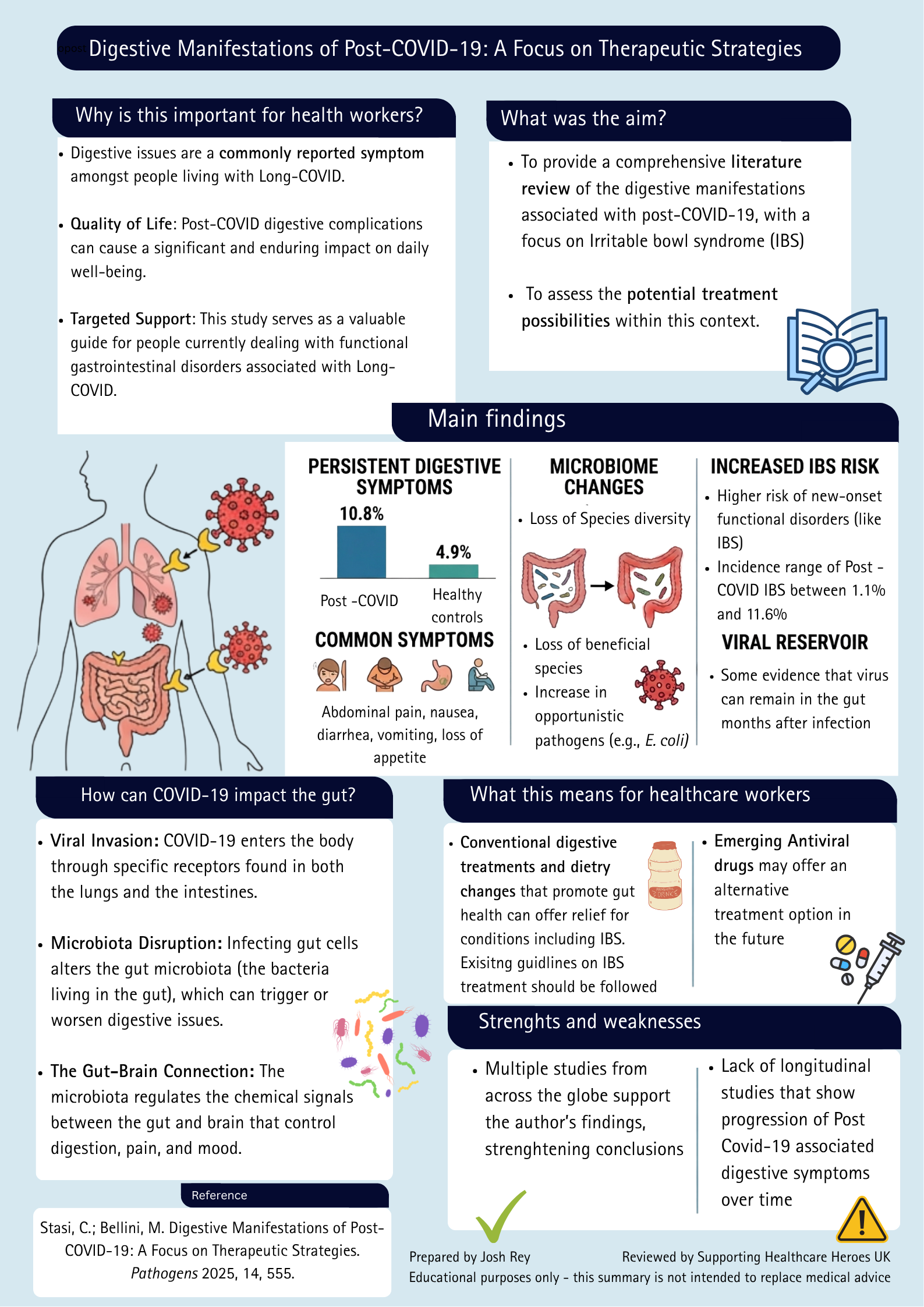
Long COVID and Digestive Symptoms: What the Research Tells Us
Research summary exploring digestive manifestations of Long COVID, including gut microbiome changes, IBS risk and potential treatment approaches.
Read more

Summary
Blog honours frontline healthcare workers, exposing PPE failures, RIDDOR under-reporting, and urges fair recognition & support for occupational COVID exposure.
This week’s blog is written by @SafeDavid3.

A previous version of this blog was published on the Patient Safety Learning website.
Those of you who watched the recent BBC Panorama programme, ‘Forgotten heroes of the Covid frontline‘ will have been appalled at the scandal that now confronts so many frontline staff for whom we stood outside our front doors and clapped so enthusiastically back in those dark days at the height of the pandemic.
This blog is dedicated to those ‘forgotten heroes’.
I hope that it demonstrates that they are not, in fact, forgotten.
I hope that the resources linked to this blog may be of help to them.
The BBC Panorama programme, Forgotten heroes of the Covid front line, touched on a number of important issues, which I will briefly summarise.
The Government (and World Health Organization) claimed that Covid-19 was spread by droplets from the nose and mouth of infectious patients, which would quickly fall to ground within two metres. Many eminent scientists across the world warned that the disease is also spread by a more insidious mechanism known as ‘airborne transmission’. This refers to tiny aerosols that hang in the air and can cause infection by inhalation. But these warnings were ignored.
It doesn’t take a rocket scientist or a competent epidemiologist to appreciate that these brave people were at considerable risk of catching Covid-19 themselves while caring for infectious patients in hospitals, residents in care homes, etc. We had all seen the news in February 2020 as the disease rampaged through Italy and noted, with considerable alarm, the number of healthcare workers who were dying from the disease.
The UK Government and health authorities had plenty of time to ensure that our healthcare workers were properly protected with the best possible equipment. But they weren’t. Instead of being provided with proper respirator masks, such as those known as FFP3s (Filtering Face‑Pieces), they were provided with flimsy surgical masks which (a) do not filter out the virus‑laden aerosols, and (b) do not provide a tight seal to the face, meaning that the aerosols can get in via the gaps around the edge. Anyone who has ever worn that type of mask and also wears glasses will have evidence of how the exhaled aerosols escape from the mask and mist up their glasses. What goes out, can come in…
To add insult to injury the authorities had the effrontery to refer to these masks as “personal protective equipment” (PPE), assuring workers that these would protect them from the disease.
For the avoidance of doubt: surgical masks are not designated as PPE under UK legislation. They never have been PPE and they are not fit for that purpose. Surgical masks do not protect against airborne hazards such as infectious aerosols. Those who recommended them for this purpose either knew that or should have known that.
As healthcare workers became infected with the disease, many NHS health trusts and health boards robustly denied there was any possibility whatsoever that their infections could possibly have been associated with their work. “Nothing to do with us” they said (or words to that effect). Then, once those who were so badly afflicted with the aftereffects of the disease (known as Long Covid) had been off work for a certain length of time, they were unceremoniously sacked.
As the Panorama programme revealed, it is this “denial of occupational exposure” by the NHS which is the most hurtful and vile aspect of the treatment meted out to our “heroes of the Covid frontline”. It is nothing less than a national scandal.
As a society, we surely owe it to our healthcare workers who have been harmed in this way to support them through the difficulties that lie ahead. In many cases they will have the aftereffects of Covid-19 for the rest of their lives. We should never forget that their grievous situation has arisen through no fault of their own, but is directly attributable to their selfless bravery back in the darkest days of the pandemic and the misinformation they were given about PPE.
Earlier, I mentioned resources that may be of help to those healthcare workers who wish to stand up for themselves and demand that their cases of Covid-19 be recognised as “occupational exposure” (as defined in UK law) and have their cases officially recorded and reported as required by health and safety legislation known as RIDDOR (The Reporting of Injuries Diseases and Dangerous Occurrences Regulations 2013).
There are two important points to remember:
What does RIDDOR actually require?If a disease was: (a) diagnosed by a doctor based on symptoms alone or, in the case of Covid-19, by a positive test result (since it was not always possible to see a doctor) (b) was more likely than not caught through your work, then it is reportable. Whether the employee was given no PPE, the wrong PPE or the very best PPE, it is still reportable. Whether the employer was or was not following official guidance, it is still reportable There is nothing whatsoever in these regulations that exempts an employer from making the statutory report on these grounds. |
This letter challenges the advice NHS Employers issued in the form of a flow-diagram regarding RIDDOR-reporting and explains why it was flawed and bore little resemblance to the RIDDOR regulations. In fairness, upon receipt of this letter NHS Employers replied confirming that they had removed the offending diagram and were now consulting with the Health and Safety Executive (HSE).
This letter sent to the HSE, overtly critical of the fact that they did not properly enforce RIDDOR reporting within the healthcare sector. Although this is a long letter, the intention was to set out an unassailable argument, based on the law, HSE guidance and the implementation of RIDDOR in other sectors of industry, as to why healthcare workers’ disease should be reported. The aim of this letter was not just to communicate these facts to the HSE (since they should already know them) but to provide information and assistance to any affected healthcare workers who may wish to read them.
HSE have replied to this letter, giving the following explanation:
“RIDDOR was originally drafted to capture single one-off unexpected events (accidents and incidents). It was not intended to be used in a pandemic involving thousands of instances of infection, where an employer may be required to make a judgement as to whether a worker caught the infection as a result of a workplace exposure or in the wider community.”
One would have hoped the HSE would have a better understanding of the role of RIDDOR and its origins. The Regulations have never just been about ‘accidents and incidents’. It has always been about diseases and long-term health issues – that is what the first ‘D’ in RIDDOR stands for. Neither has it been solely about ‘capturing single one-off unexpected events’, it has been about identifying trends that need further investigation.
Dating back to HSE Guidance L.73 in 1995:
“The [RIDDOR] reports alert the enforcing authorities to individual incidents. They also provide data which indicates how risks arise and show up trends.”
Had RIDDOR-reporting been properly enforced trends would (or should) have been spotted in relation to overall infection-rates among healthcare workers.
In any event, I am not persuaded that this is a valid reason for denying recognition and official recording of ‘occupational exposure’ to a lethal disease against which our healthcare workers so valiantly battled at extreme risk to their own health. It only takes a few minutes to tap the relevant details into the online RIDDOR system for each case. It is not a lot to ask.
Interestingly, whereas my concern centres around under-reporting, HSE respond by saying that:
“They have found a significant amount of over-reporting”.
I am lost for words! Please refer to the last page of my letter to them and make up your own minds.
I have prepared my own flow-diagram setting out the way in which RIDDOR should have been (and should continue to be) implemented in the healthcare sector during the pandemic. I must emphasise that this diagram represents my own personal and professional interpretation of the reporting mechanism and has no official status.
HSE will undoubtedly push back on some aspects of this, particularly the aspects of worker-to-worker cross-infection within healthcare premises which their guidance states is non-reportable. I state that it is reportable and I give my reasons. I am pleased to note that in their letter of reply they do not contest this point.
I have produced a template letter which you are welcome to download and adapt according to your own particular circumstances. You may want to send it to your Trust, health board or other employer, setting out your reasoning as to why your case is, even now (may be a year or two after their initial infection), RIDDOR-reportable.
I have also provided some guidance notes to assist you in using the template letter:.
Even if this letter fails to persuade the more intransigent health trusts/boards to RIDDOR-report (and one can anticipate them being instructed by HSE not to), such a letter may be helpful in demonstrating ‘occupational exposure’ in the event healthcare workers eventually become eligible for some form of State support which they so richly deserve.
Healthcare workers have not been, and are still not, treated fairly or ethically by the Government, their Departments and Agencies or their own employers. Health and Safety legislation is not being applied equitably between the healthcare sector and other industry sectors. This applies both to the regulations known as COSHH (relating to safe working with hazardous substances, including pathogenic organisms), where the basic requirements for respiratory protection have not been met, and RIDDOR (as described above), where it is basically a postcode lottery as to whether healthcare workers’ COVID-19 infections are recognised and recorded as ‘occupational exposure’ or not.
Going forward, to strike a more positive note, my greatest hope is that a just and fair arrangement is put in place to support those healthcare workers whose lives have been ruined through their selfless devotion to duty during the pandemic. It matters not whether this is achieved via the Industrial Injuries Disablement Benefit scheme or a bespoke scheme comparable with the Armed Forces Compensation Scheme for injured veterans. After all, throughout the pandemic we have referred to them as “frontline workers”.
David Osborn is a chartered occupational safety and health practitioner, having been in practice for 28 years. He has a background in biochemistry, microbiology, epidemiology and emergency planning.
David provides support to the Covid Airborne Transmission Alliance (CATA), a core participant at the UK Covid Inquiry. CATA is a consortium representing over 65,000 healthcare workers. However, any blogs or letters that David writes to Government departments, Agencies or the NHS are written entirely on a personal and individual basis.
Research summary exploring digestive manifestations of Long COVID, including gut microbiome changes, IBS risk and potential treatment approaches.
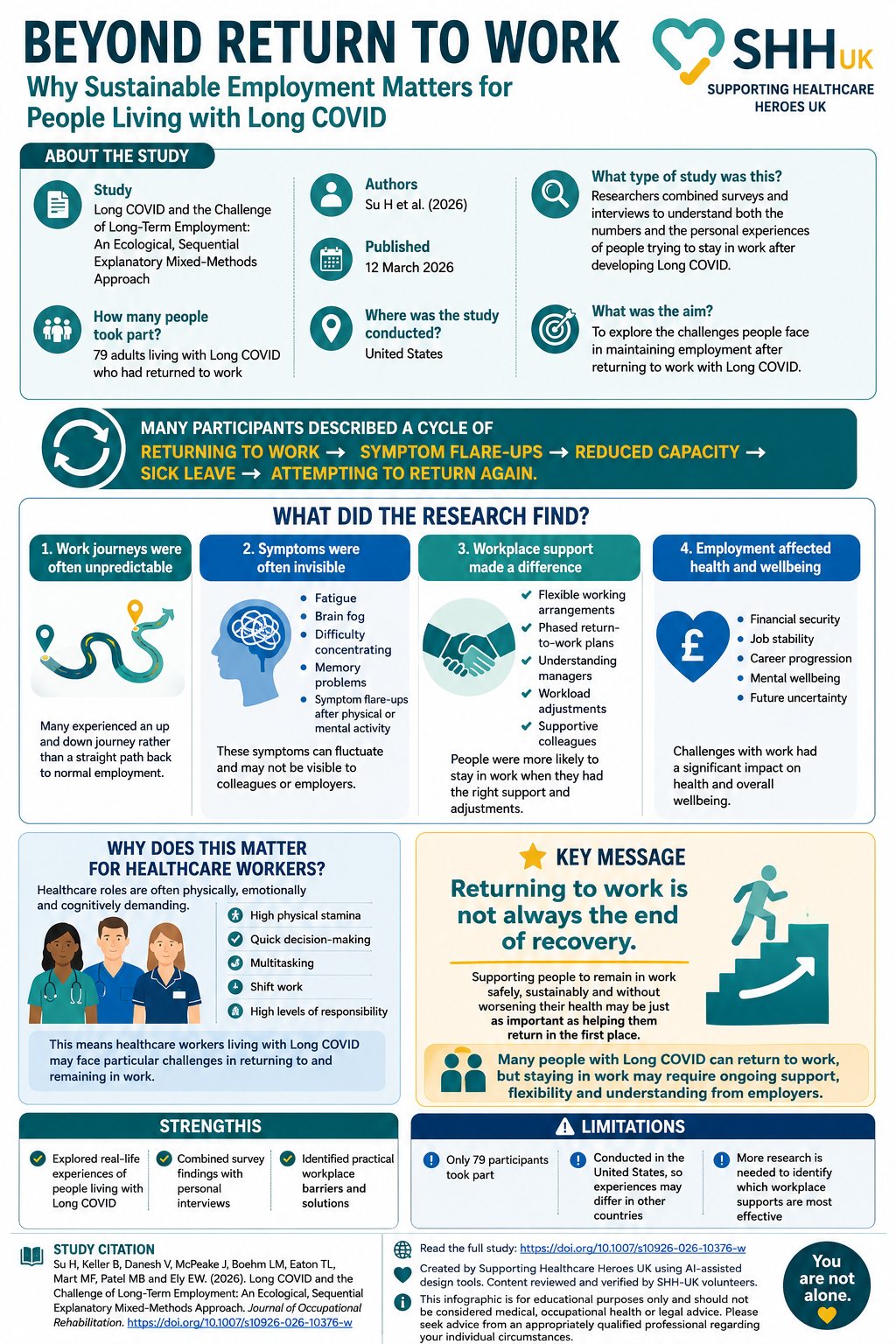
Returning to work is often viewed as a major milestone in recovery. However, for many people living with Long COVID, returning to work does not necessarily mean returning to their previous level of health. This study by Su and colleagues explored the experiences of 79 adults living with Long COVID who had returned to employment. […]
Learn why the precautionary principle is fundamental to infection prevention and how its application protects healthcare workers and patients.