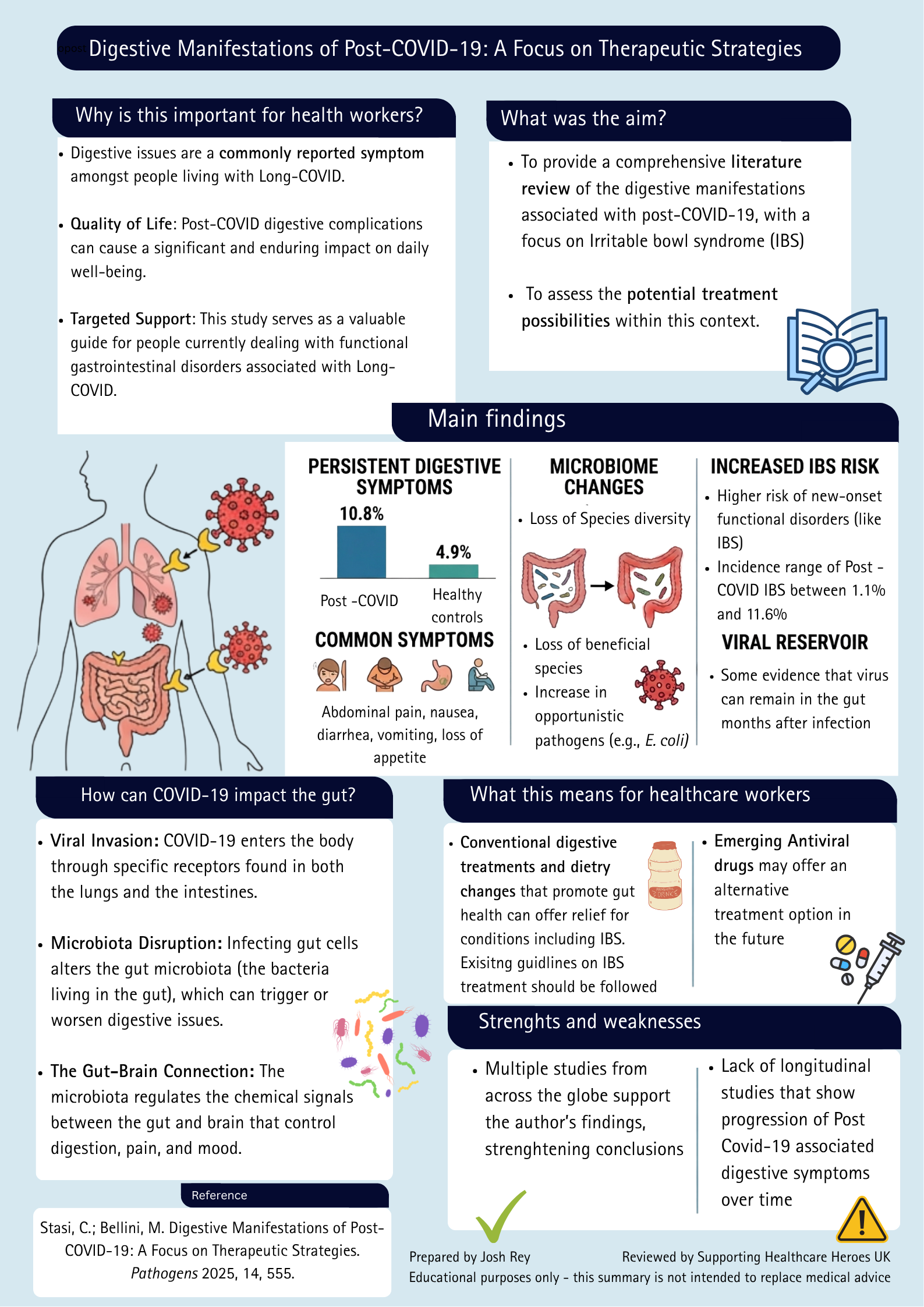
Long COVID and Digestive Symptoms: What the Research Tells Us
Research summary exploring digestive manifestations of Long COVID, including gut microbiome changes, IBS risk and potential treatment approaches.
Read more

You must not be given unsafe care or treatment or be put at risk of harm that could be avoided.
Figure 1: The first tweet
 For the first NHS Trust to meet this fundamental standard, and for there to be safety going forward with reduced mask usage, there would need to be zero nosocomial covid infections at present, and an assessment that reducing controls would present no additional risk.
A reference table of nosocomial transmission is produced and tweeted weekly* from NHS data. For the first Trust, (Norfolk and Norwich Universities Foundation Hospitals Trust) the nosocomial rate is about halfway down the table. In the last 28 days prior to reporting (30th March 2023), there were 198 people in the Trust of whom 64 (32%) acquired SARS-CoV-2 in the Trust. Therefore, every day, at least 2 people get hospital acquired COVID-19 in the Trust. Its on a par with the overall result for all the Trusts – but it’s not good. With this level of acquisition (which of course does not include staff acquisitions or those detected post discharge), it will be impossible to reduce mitigations further and meet the Fundamental Standard as two people are already harmed every day by acquiring COVID-19. The logical assessment would be that more will be harmed if additional controls are reduced.
The Trust’s tweet also informs that local risk assessments will be in place, e.g., masks will be worn when caring for “immunosuppressed patients”. The question is how they will know everyone in hospital who is immunosuppressed prior to beginning their care. That seems an impossible task. For example, the immunosuppressed people will have to first have a conversation with the unmasked member of staff, before they put a mask on. The plan therefore is to live with an unacceptable level of nosocomial COVID-19 and to further reduce measures which can only facilitate a higher rate. The plan to protect vulnerable people does not seem fool proof. Thus, the Trust’s plan appears to fail the Fundamental Standard of care. The Trust is putting more people at risk of harm rather than reducing the numbers exposed daily to an airborne infection.
For the first NHS Trust to meet this fundamental standard, and for there to be safety going forward with reduced mask usage, there would need to be zero nosocomial covid infections at present, and an assessment that reducing controls would present no additional risk.
A reference table of nosocomial transmission is produced and tweeted weekly* from NHS data. For the first Trust, (Norfolk and Norwich Universities Foundation Hospitals Trust) the nosocomial rate is about halfway down the table. In the last 28 days prior to reporting (30th March 2023), there were 198 people in the Trust of whom 64 (32%) acquired SARS-CoV-2 in the Trust. Therefore, every day, at least 2 people get hospital acquired COVID-19 in the Trust. Its on a par with the overall result for all the Trusts – but it’s not good. With this level of acquisition (which of course does not include staff acquisitions or those detected post discharge), it will be impossible to reduce mitigations further and meet the Fundamental Standard as two people are already harmed every day by acquiring COVID-19. The logical assessment would be that more will be harmed if additional controls are reduced.
The Trust’s tweet also informs that local risk assessments will be in place, e.g., masks will be worn when caring for “immunosuppressed patients”. The question is how they will know everyone in hospital who is immunosuppressed prior to beginning their care. That seems an impossible task. For example, the immunosuppressed people will have to first have a conversation with the unmasked member of staff, before they put a mask on. The plan therefore is to live with an unacceptable level of nosocomial COVID-19 and to further reduce measures which can only facilitate a higher rate. The plan to protect vulnerable people does not seem fool proof. Thus, the Trust’s plan appears to fail the Fundamental Standard of care. The Trust is putting more people at risk of harm rather than reducing the numbers exposed daily to an airborne infection.
Figure 2: The second tweet
 They tweet “air filtration units are now on our wards and clinical areas.” As there are different approaches here, the question is which of these Trusts is following the National Infection Prevention and Control Manual (NIPCM) to keep people safe. The manual specifies that SARS-CoV-2 is, spread by droplets, unless there is an aerosol generating procedure performed when it is spread via aerosols. There is a reference to a ‘Note Above’ for further details. Here is the note:
There is a red flag in the first line:
They tweet “air filtration units are now on our wards and clinical areas.” As there are different approaches here, the question is which of these Trusts is following the National Infection Prevention and Control Manual (NIPCM) to keep people safe. The manual specifies that SARS-CoV-2 is, spread by droplets, unless there is an aerosol generating procedure performed when it is spread via aerosols. There is a reference to a ‘Note Above’ for further details. Here is the note:
There is a red flag in the first line:
“the distinction between droplet and aerosol transmission is not always clearly defined.”It’s a red flag because exhalations produce both aerosols and droplets. Also, pathogens are not sentient beings; they cannot decide whether to jump into large or small particles. There is also a missing statement – the need to continuously strive to reduce nosocomial acquisitions. The ‘note’ further states the need for a ‘dynamic clinical risk assessment’ which should include “an evaluation of the ventilation in the area”. However, there is no instruction as to what level of ventilation should initiate any specific action. Respirators are to be used “when deemed necessary after the risk assessment.” Again, what finding initiates this action is unspecified. What should also be stated is whether the risk assessment is to prevent transmission from a known case, to stop an outbreak, or to create a space where the risk to all people therein is minimal should there be unknown infectious people present. For safety, I offer an amended ‘note’ (Table 1). Table 1: Amended note
| SARS-CoV-2 is spread via the airborne route mainly close to the infectious source, but also at distance when ventilation is poor |
| It is exhaled and inhaled in aerosol particles ≤100μm regardless of any aerosol generating procedure. Closeness to the source is of paramount importance to acquisition, i.e., within stethoscope rage and the distance wherein nurses nurse. |
| NB it is not always a risk that can be easily identified, therefore as we look after people in congregate settings, we must endeavour to make all environments safe for all people. |
| Although the disease is less pathogenic than when the pandemic first began (due to vaccines), it is still a significant disease-causing pathogen and can cause damage to any system in the body. |
| Long term sequalae are also a significant risk for everyone. |
| Avoidance of infection and avoidance of repeat infections are to be promoted by using airborne precautions and standard precautions. |
Although people are exposed to acquisition outside of hospital – we must endeavour not to expose them when they enter our facilities. It is vital that clinically vulnerable people, who are at a much higher risks of negative outcomes are protected. To that end each organisation must take the steps outlined in Table 2.
Table 2: Steps needed to protect people from exposure to Covid-19 during a hospital visit
| Work to assess and provide Indoor Air Quality (IAQ) in all clinical and non-clinical areas using a range of specialists who will identify and prioritise places with poorer air quality for improvement. |
| Have and follow a plan to ensure the safety of all people, especially those who are clinically vulnerable. |
| Place patients in clinical areas where they will not present a risk of harm to others and where others will not present a risk of harm to them. |
| Investigate, learn, and optimise care and ventilation when nosocomial cases are identified. |
| Use respiratory protection equipment (RPE) when caring for anyone considered infectious with or suspected of having SARS-CoV-2. |
| Use their ongoing COVID-19 acquisition data to adapt their respiratory protection equipment policies and protections to ensure an ongoing reducing rate (in both staff and patients). NB RPE will always be required for caring for people with SARS-CoV-2. |
| Areas presenting the highest risk with poorest IAQ should be tackled first. |
The above has a lack of ventilation specifics because IPC people (like me) are neither trained, nor have expertise, in ventilation. This must be deferred to the experts – aerosol scientists and engineers – whose role in the environmental controls of this airborne virus should have been established long ago. Specifications for maintaining IAQ for each clinical area are critical to preventing ongoing transmission.
So, the East Suffolk and North Essex Trust, have an ongoing nosocomial COVID-19 incidence which they are tackling by improving indoor air quality (IAQ) for this airborne virus. It is more than the NIPCM specifies, because the NIPCM fails to state SARS-CoV-2 is airborne and offers no help or recommendation for IAQ other than a do-it-yourself risk assessment.
The Norfolk Trust is reducing mitigations in their hospitals. This appears an erroneous assumption of safety. We should not reduce COVID-19 precautions unless we can guarantee it is safe to do so. We must meet the Fundamental Standard by actions that do patients no harm. The different approaches indicate that the NIPCM appears inadequate to guide Trusts to safe decision-making. Finally, zero nosocomial transmission would seem a good place to be before reducing control measures.
This may seem ridiculously optimistic or outdated given precautions outside of hospitals have all but disappeared. However, COVID-19 continues to be the cause of long-term ill-health. It depletes our staff by sickness and absences. It still kills hundreds of people a week and hospitals look after infectious people as well as the most vulnerable – we must protect them all.
*@lawtontri produces a table of nosocomial acquisitions of SARS-CoV-2 every week on twitter
Research summary exploring digestive manifestations of Long COVID, including gut microbiome changes, IBS risk and potential treatment approaches.
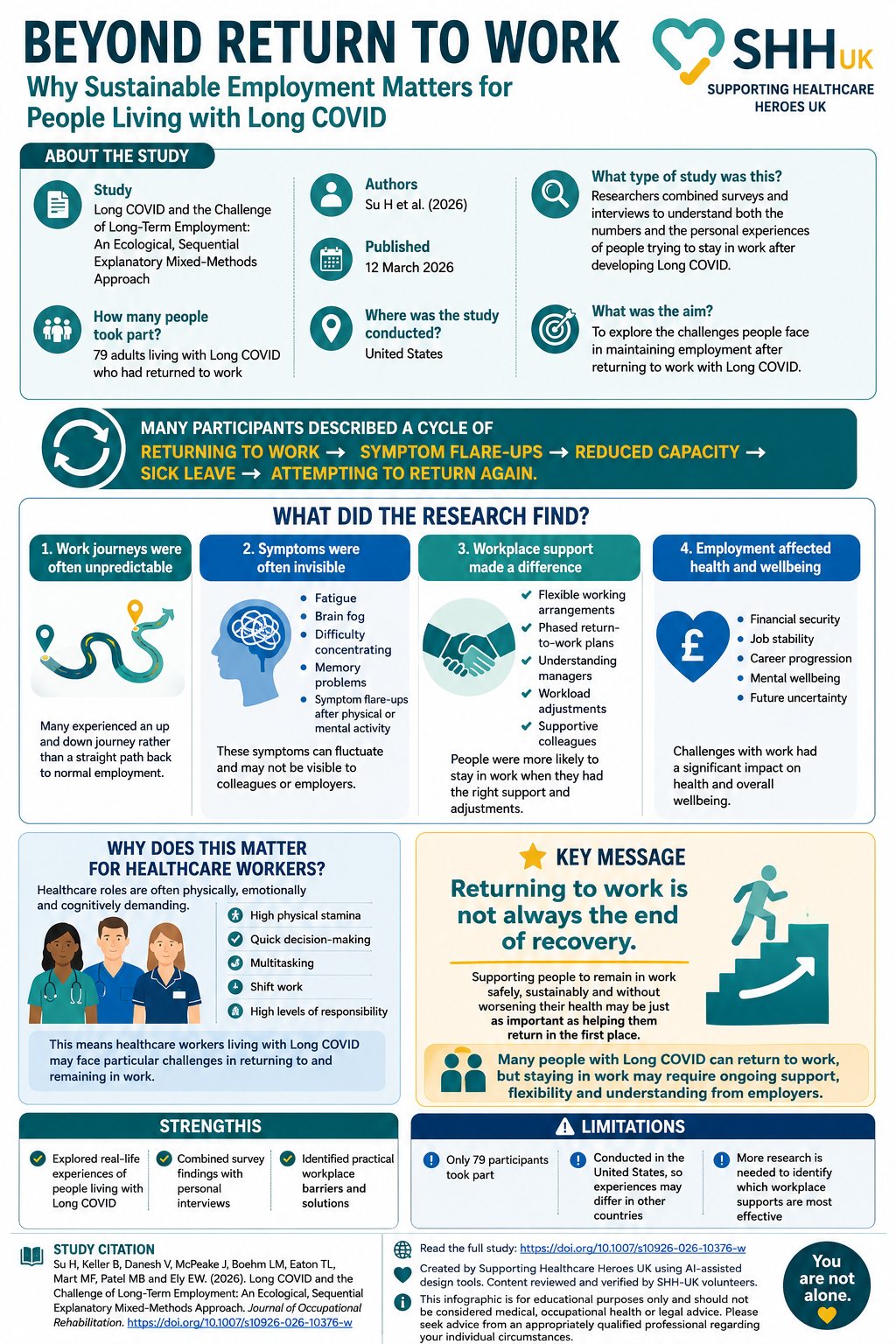
Returning to work is often viewed as a major milestone in recovery. However, for many people living with Long COVID, returning to work does not necessarily mean returning to their previous level of health. This study by Su and colleagues explored the experiences of 79 adults living with Long COVID who had returned to employment. […]
Learn why the precautionary principle is fundamental to infection prevention and how its application protects healthcare workers and patients.
David Osborn says:
A very interesting article which brings home just how much of a ‘postcode lottery’ your safety whilst in hospital can be.
From their web page about this, the NNUH Trust apparently underpinned their decision to remove mask wearing rules by conducting risk assessments. Since, by law, risk assessments must be recorded in writing, a request has been made to publish these documents via a Freedom of Information Request.
For anyone interested in following this line of inquiry, the FoI may be found here:
https://www.whatdotheyknow.com/request/change_to_face_mask_guidance_3_a#outgoing-1448863
Their response should be available online at the above link (by scrolling down on the page) by 16th May 2023.